
Wounds, battlefield trauma, and their survivability in the British Civil Wars
This week’s blog is the second in a trilogy of blogs which have been written for us by our colleague Professor Stephen M. Rutherford of the School of Biosciences, Cardiff University. His previous blog used examples drawn from Civil War Petitions to illuminate the nature of the physical damage inflicted on the body by gunshot wounds sustained during the Civil Wars. This instalment uses the evidence from Civil War Petitions to discuss the tricky issue of surgical effectiveness and survivability…
Corporal John Barret of Captain Cotton’s Company, on the Parliamentarian side in a skirmish at Painswick, Gloucestershire, 1644, suffered a horrible fate at the hands of the enemy. Shortly afterwards, he reported to the Parliamentarian Governor of Gloucester, Colonel Edward Massey (signed Massie in the petition), who then endorsed his petition, that he had been set upon by two cavalrymen and six infantrymen, whereupon he was cut ‘downe and left for dead: and having receaved Tenne wounds of them [they] stript me starck nacked to the very skine’. He reported that ‘ever since that time I have layne bedrid under the Cyrurgions hands and now I being able to rise I can not for want of Cloths’. Colonel Massey confirmed that John had ‘receved 7 wounds in the head 5 of them therow the scull [one] cut in the backe (to the bons [bones]) with a pole axe his elbow cut off bons and all: his hand slitt downe betwine the fingers.’ We do not know whether Corporal Barret survived these wounds long-term, but he certainly survived long enough to make the petition, and described his effective treatment: ‘Mr Caradine the Cyerrugion [surgeon] afermeth who hath almost Cured them al (and very car[e]fuly and willingly he hath taken the pains to do it) how to satisfie him we know not he was never the man that asked us a farthing.’ The extent of Corporal Barret’s wounds were extreme – including scalping the skull down to the bone, as well as a bone-deep cut in the back, several other wounds, and the loss of an arm. The fact that he did not die on the battlefield is remarkable, but the fact that he survived long enough to petition the Governor for clothes and means to repay the surgeon show clearly the capability of surgeons in the British Civil Wars. The injuries treated by Mr Caradine were more extreme than some modern day military wounds, and yet he lived to tell the tale.
Ambroise Paré (credit: Wellcome Collection)
Surgeons and physicians in the early modern period have gained a reputation in the popular mind as savage butchers with little or no understanding of medicine. However, recent historiography in this area – especially the work of Ismini Pells on Civil War military surgeons (Pells, see also Rutherford, 2016 and 2018) has highlighted that surgeons in this period did undertake procedures that had substantial merit in biomedical terms. Indeed many of the procedures pioneered in this period are still in use in modern military medicine today (Rutherford, 2018). Far from being unskilled and ineffective, there is evidence of early modern surgeons practicing a form of ‘Evidence-based Medicine’. That is using empirical evidence of their experiences and reports to guide and refine medical practice. Such practitioners included Ambroise Paré, sixteenth-century surgeon to the Kings of France, James Cooke, Parliamentarian surgeon during the Civil Wars, and Richard Wiseman, personal surgeon to Charles Prince of Wales, and later Sergeant Surgeon to him as King Charles II.
The following video demonstrates the extent to which a cheap sword, quality sword, and dagger could injure a human limb (the video uses a leg of meat as an equivalent substitute):
From this video you will see that even a cheap, mass-produced sword wielded by an inexperienced swordsman, could potentially cut several inches into an unprotected limb. A heavier, better quality sword was capable of a cut of 10-15cm in depth, and about 20cm in width – easily sufficient to sever a limb or cut into an unprotected skull. Battlefield archaeology from earlier conflicts, such as the Battle of Towton in Yorkshire (1461), or the Battle of Visby in Sweden (1361), display numerous examples of severed limbs and cuts deep enough to slice or shatter bone. Even if the limb was not shattered, the cut would be deep enough to make repair difficult or potentially impossible. The challenge to a military surgeon, therefore, was considerable.
Without the proper medical records it is not possible to determine the survival rate of injuries suffered by Civil-War soldiers. What can be inferred, however, is some degree of effectiveness of surgical procedures from the evidence of the extent of wounds survived by Civil-War soldiers. In the archaeological finds mentioned above, there were examples of skeletons of persons surviving quite catastrophic injuries (severed or broken limbs, sword cuts deep enough to scar the bone, for example) long enough for those injuries to heal and the bones to fuse or produce new growth. The petitions uncovered and transcribed as part of this project give some valuable insights into both the wounds suffered by soldiers (and some civilians) in the Civil Wars, and also the extent to which these wounds were potentially survivable, after effective medical care.
For example, the certificate for William Gray of Braintree, Essex, (8 April 1657) reported that he was ‘very much Debilitated in his limbs’, and that his ‘Legge hath beene brocken in many peeces’, and yet appears to have healed sufficiently for it not to need to be amputated. Another petitioner, John Ellis, of Dewsbury, in the West Riding of Yorkshire, reported (October, 1674) that he had received ‘received severall Wounds in severall partes of his body’, claiming that these had made him ‘impotent, lame and [decrepid] not able to worke for a livelihood’. William Sudbury of Woodnewton, Northamptonshire was reported (while requesting an increase to his pension, Trinity, 1674) to have received ‘13 wounds in his head & body very dangerous, but also the fingers of one of his hands cut [off]’. These substantial injuries disabled William from making a living, but the fact that he was able to survive such extreme damage to his body is quite remarkable. David ap Jevan of Bersham of Denbighshire (certificate dated 20 September, 1663) also had digits cut from his (left) hand, sufficient wounding to stop him being able to make a living for himself, but a wound that he survived for at least 20 years after his initial injury (at Holt Bridge in November 1643). These would have been wounds received on a dirty battlefield, and which would have been treated either in situ, or close by at a lodging. The patient would need to survive potentially catastrophic blood loss and shock at the moment of injury, and then also survive the potential infection of the wound at a time long before the discovery of antibiotics.
A review of the approaches adopted by early modern surgeons (in particular military surgeons) highlights that there was a good level of understanding about suturing or bandaging of wounds, and the control of post-operative infection. There were a range of different suture methods, described by authors, such as Wiseman and Cooke, each with a specific wound type to be used for. There was also a range of ligatures (use of bandages to seal wounds) adopted as an alternative approach. Antibacterial agents, such as alcohol or posca (a water/vinegar mix) were used on equipment and bandages. Egg albumen or honey (the latter’s high-sugar concentration being a natural antibacterial agent) were used as salves to keep the wound healthy. Even though in the seventeenth century there was no understanding of the biology behind microbial infections, the surgeons were aware of the effectiveness of these approaches, and even disdainful of other, less-effective methods.
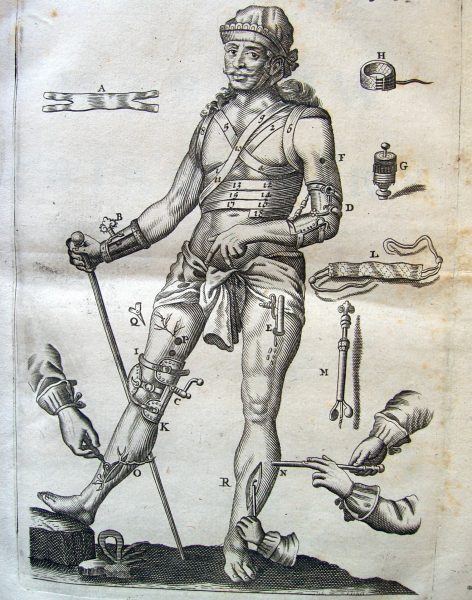
Image from James Cooke’s surgical treatise Mellificium Chirurgiae
The efficacy of many of their approaches has stood the test of time, and are still in use in modern medicine. For example, in the post-operative management of infections, a common strategy was to leave the wound un-sutured and open for several days, the tissue kept apart by a ‘tent’ (a roll of bandage inserted into the cut). The wound was left until the flesh was ‘like flesh long hang’d in the air’ (Wiseman, p. 428). This approach, termed in modern medicine ‘delayed primary closure’ is in common use today for the treatment of conditions such as appendicitis, compartment syndrome, and some military injuries, most recently in the wars of Afghanistan and Iraq (Leininger, Rasmussen, Smith, Jenkins and Coppola). This approach for encouraging the body to treat its own infection (the theory – which even today is not confirmed – is that the open wound encourages the flow of lymph, which in turn encourages that accumulation of white blood cells and stimulates the immune response at the wound site) is seen in medical manuals from the mid-sixteenth century, and in manuals from numerous major conflicts over the subsequent centuries (Rutherford, 2016).
Recovery from extreme injuries was slow and uncertain. Details of the extensive hospital care provided to some soldiers in the Civil Wars have been researched extensively by Eric Gruber von Arni, who revealed what was often an organised and systematic process of patient care, not least of which was the high calorific intake for patients, to aid their recovery. But the experience recorded in the certificate for Thomas Wayte of Doncaster in the West Riding of Yorkshire (March 1668) illustrates the extensive nature of this recovery period. It was reported that Thomas ‘resaiued [received] such desp[e]rate wounds, that he lay most dangerously on them for three or foure years together.’ This long-term need for care, and the requirement for support of disabled soldiers after their recovery, was frequently down to their families and community, as Ismini Pells and David Appleby have discussed in their blogs on this website: ‘Old Wives’ Tales: Long-term Medical Care during the English Civil Wars’ and ‘Members of one another’s miseries’: care in the community during and after the Civil Wars’.
It is clear from these petitions that soldiers did survive catastrophic and life-changing injuries, often living with them for decades after they were inflicted. The physical and mental challenges of living with disabilities caused by traumatic injuries would have been considerable. It is remarkable, however, that soldiers with such extensive injuries survived at all, and a re-evaluation of the medical practices, and their effectiveness, of early modern surgeons has the potential to reveal significant insights into the development of surgical procedures, and the extent of their medical validity. It is a trope that ‘war drives innovation’, and this may well be true for the pioneering surgeons and medical practitioners in the British Civil Wars. One wound type, mentioned in my previous blog, that was of major significance in the Civil Wars was injury from gunshots. Injuries from such wounds were another challenge entirely, and the third blog in this series will look at the approaches taken for their treatment.
References and further reading
For further reading into the practitioners of medicine and surgery in the sixteenth and seventeenth centuries, an excellent resource is the Early Modern Medical Practitioners Project at the University of Exeter. This project has a range of different foci on early modern medicine, including cataloguing as many examples of named medical practitioners as can be identified.
Primary Sources
J. Cooke, Supplementum Chirurgiae, or the supplement to the Marrow of Chyrurgerie (London, 1655).
J. Cooke, Mellificium Chirurgiae, or the Marrow of Chirurgery much enlarged (London, 1676).
A. Paré (T. Johnson, translation), The workes of that famous chirurgion Ambrose Parey translated out of the Latine and compared with the French (London, 1634).
R. Wiseman, Severall Chirurgical Treatises (London: Norton and Maycock, 1676).
Secondary Works
E. Gruber von Arni, Justice to the Maimed Soldier: Nursing, Medical Care and Welfare for Sick and Wounded Soldiers and their Families during the English Civil Wars and Interregnum, 1642–1660 (Aldershot: Ashgate, 2001).
B. E. Leininger, T. E. Rasmussen, D. L. Smith, D. Jenkins and C. Coppola, ‘Experience with Wound VAC and Delayed Primary Closure of Contaminated Soft Tissue Injuries in Iraq’, Journal of Trauma Injury, Infection, and Critical Care, 61 (2006), pp. 1207-11.
I. Pells, ‘Reassessing frontline medical practitioners of the British Civil Wars in the context of the seventeenth-century medical world’, The Historical Journal, 62:2 (2019), pp 399-425.
S. M. Rutherford, ‘Ground-breaking pioneers or dangerous amateurs? Did early-modern surgery have any basis in medical science?’, in I. Pells (ed.), New Approaches to the Military History of the English Civil War (Stroud: Helion and Company, 2016), pp. 153–85.
S. M. Rutherford, ‘A new kind of surgery for a new kind of war: gunshot wounds and their treatment in the British Civil Wars’, in D.J. Appleby and A. Hopper (eds), Battle-Scarred: Mortality, Medical Care and Military Welfare in the British Civil Wars (Manchester: Manchester University Press, 2018), pp. 57-77.
John Balshaw's Jigge: Singing, Star-Crossed Lovers and Signing a Civil War Petition

'Meamed and Lamed': Approaching Civil War Petitions through the Lens of Disability History

‘Lost and impoverished for ever’: The effect of the Civil Wars on Local Communities as seen through Civil War Petitions

Civilian Suffering in the Civil War: the case of Tysoe in Warwickshire

'Battle-Scarred': The Civil War Petitions Summer School
The Persistent Petitioner: Mary Burden, Oliver Cromwell and the Wiltshire Justices of the Peace
‘The hungry jaws of want’ – Basing House and the Maw of War

'The endeavours of your servants': Oliver Cromwell, Military Welfare and Civil War Petitions
A Vengeful Vicar and a Martyred Mother: The Petition of James Bamlett
