
The personal cost of war: injuries from firearms and their treatment during the Civil Wars
This is the final instalment in our trilogy of blogs on medical care written for us by Prof. Stephen M. Rutherford of the University of Cardiff. It combines the themes from the first blog examining the physical impact of gunshot wounds with the themes from the second blog examining surgical effectiveness and survivability, to uncover how surgeons during the Civil Wars treated wounds from firearms during the Civil Wars…
John Woodall.: line engraving by G. Glover, 1639 (image from the Wellcome Collection, reproduced under a CC-BY 4.0 licence).
In his treatise on gunshot wounds published in 1628, John Woodall remarked that ‘No wound of Gun-shott can be said to be a simple’, a maxim that was eloquently reinforced by the experiences of soldiers in the British Civil Wars nearly two decades later. A substantial number of petitions in this project refer to wounds from firearms (muskets, pistols and/or cannon shot), many of which were serious enough to cause long-lasting disability, such as the loss of use of a body part (or actual loss in some cases), or chronic debilitating pain in an injured part of the body. For example, the case of Michell Powell of Wrexham, Denbighshire (10 July 1660), whose petition reported that he had been ‘shott in the right arme though beinge partly cured then: yett in the p[ro]cess of tyme festered agayne & soe corrupted yt it grew to be a woolfe or gangrene … payinge the Chyrurgion for cuttinge the sayd wolfe forth & beinge still in a lamentable Condyc[i]on through deadnes of flesh: hauinge his veynes & nerues shrank & knotted through the dolor therof’. This petitioner was rendered unable to work as a result of this wound, leading to extreme hardship: ‘hindred yo[u]r poore petyc[i]oners callinge beinge a taylor & hauing 5 smal children soe yt his wyfe was constrained to wander about the towne to collect the charytie of all well disposed people’. This petition demonstrates the severity of the wound, but also its subsequent physical and financial impact.
Some wounds from firearms could be very extensive. The petition of former royalist soldier, Edward Bagshaw, of Conisbrough, West Riding of Yorkshire (3 August 1668) recorded that he was shot in the side of the body, but also received ‘many wounds & cutts in the head in somuch that yo[u]r petic[i]on[e]r had nine bones taken out of his skull, And all that nourished yo[u]r petic[i]on[e]r for three weekes he rec[eiv]ed in att a hole in the side of his head …’. With many conflicts being assaults upon, or siege actions of, towns and cities, soldiers were not the only victims of injuries from firearms. An unusual petition came from Jane Merrick of Upton Bishop, Herefordshire (dated 1661 to 1662), who reported that she herself was wounded by a cannon ball: ‘yo[u]r pet[itione]r when the scotts beseiged this Citty was wounded by a Cannon shott in th legg when as she was a doeinge servis for this Cittie a makeinge vp a breach w[hi]ch was in Wigmore streete’. Jane was so badly injured that she needed to be carried to safety by ‘Mr Hugh Rodd’ (for more on Merrick, see this previous blog by Lloyd Bowen).
The damage from bullets was not the only danger. The gunpowder itself was also a significant risk, as most muskets used in the Civil Wars were matchlock muskets, loaded with loose back powder, and fired using a piece of burning ‘match’ cord. Royalist surgeon Richard Wiseman recalled the case of a musketeer, whose store of gunpowder ignited while filling his bandoliers (a strap across the body from which hung small wooden bottles, each containing sufficient loose gunpowder to load and fire the musket once) with disastrous consequences:
‘A Souldier in the time of service being in the Fort-Royall at Worcester, hastily fetched his Bonnet full of Gun-powder; and whilst he was filling his Bandeliers, another Souldier carelesly bestrides it, to make a Shot at one of the Enemies which he saw lying perdue. In firing his Musket, a spark flew out of the Pan, and gave fire to the Powder underneath him, and grievously burned the Hands, Arms, Breast, Neck and Face of him that was filling his Bandeliers. And as to himself, he likewise was burned and scorched in all the upper part of his Thighs, Scrotum, the Muscles of the Abdomen, and the Coats of the Testicles to the Erythroïdes, so that the Cremasters were visible. And indeed it was to be feared, that, when the Escar should cast off from his Belly, his Bowells would have tumbled out.’
The majority of wounds from gunshot, however, were likely to have been caused by the damage made by the entry of the musket ball (variously also termed the ‘bullet’ in primary sources). See the first blog of this trilogy for details of musket ball damage. Gunshot wounds were no longer novel, by the time of the Civil Wars, and had been described in published works by surgeons such as Thomas Gale (1563), William Clowes (1588), and John Woodall (1628, 1655). However, one might argue that the duration of civil-war conflict provided unprecedented numbers of this wound type in the British Isles. The longevity of the published works of two civil-war surgeons, James Cooke and Richard Wiseman, demonstrates the significance of their procedures. Wiseman’s opus, Severall Chirurgicall Treatises (1676), was reprinted in five editions up to 1745, and his work was still cited as the leading authority on gunshot wounds in Ballingall’s Outlines of Military Surgery (1844).
While some treatments were effective, equally there were some wounds that were beyond help, as Wiseman recounted regarding one unfortunate patient who had been treated by another surgeon:
‘In the Wars I was called to see a poor Souldier, who had his Arm shot off near the Shoulder. The bruised and shattered Stump seemed to his Chirurgeon to be gangrened, and accordingly he drest him with Aegyptiac. as a Gangrene: from which sharp Dressings the Wound gleeted, and, by reason of the Pain, inflamed. He had roared some days through the vehemency of that Pain. When I came to him, I saw a great Trembling of the Part, and a frequent twitching upwards of the Tendons and Musculous flesh in the Stump; also the Flesh in the whole Stump was of a whitish colour, as if it had been scalded.’
The state of this wound was critical, and on this occasion, despite trying to control the deterioration of the tissue, Wiseman noted ‘but it was too late, he died howling’. This unfortunate soldier might have survived had his early treatment been different, since within the petitions shared by this project, there is evidence of similar wounds that were survived.
The first blog in this series describes the physical damage caused by a musket ball. But how was this damage treated? The ball would penetrate the body causing internal damage via ‘permanent’ and ‘temporary’ cavities. However, unlike modern bullets, often there was no ‘exit wound’ from a musket shot, as the soft lead musket ball would potentially flatten or be diverted from its trajectory within the body. In this case, the surgeon would need to remove the bullet as part of the treatment. First the bullet needed to be found, a procedure best done by the surgeon inserting his finger, or a long metal probe, into the wound. The feel of metal touching metal was different to that of metal touching bone or sinew, and so a metallic bullet could be located using this method. On some occasions the outline of the embedded musket ball could be seen under the skin, in which case making a new incision in the patient was easier and safer for removal. Most commonly, the bullet was deep within the body tissues, and so needed to be removed the way it came in. Two forms of implement were used for retrieval. Firstly a ‘tirefond’ or ‘terebellum’ bullet extractor, which was a long thin implement, with a central baffle ending in a screw thread. The instrument could be inserted into the wound, and the screw-tip then drilled into the soft lead of the ball, before removal from the body. Alternatively, long forceps or pliers could be used, of which there was a wide diversity of shapes and modes of action, typically given descriptive names such as a ‘crow’s bill’, ‘crane’s bill’ and ‘lizard mouthe’ (Rutherford, 2018).
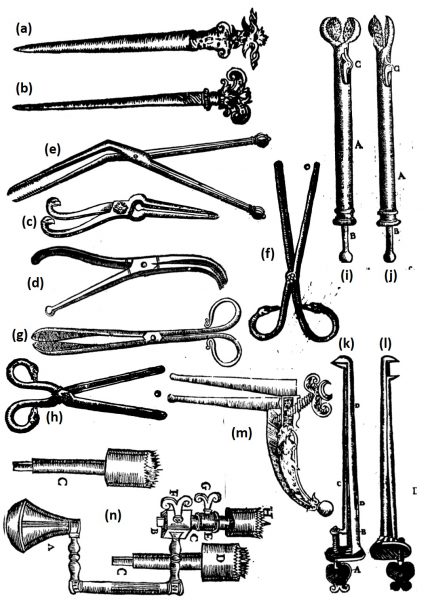
Surgical implements. (a,b) Tirefond bullet extractors, (c,d) Crowe’s Bill, (e,f) Crane’s Bill, (g,h) Drake’s Bill, (i) Catch-bullet and (j) Lizard’s Mouthe articulated bullet extractors, (k,l) Parrot’s Bill, open and closed respectively, (m) Swan’s Beake, (n) Trepanning tool showing fittings. Not shown to scale. Composite of images from T. Johnson, The workes of that famous Chirurgion Ambrose Parey (1634), pp. 366 (n), 419 (c), 420 (e,f,h,i), 421 (j-m), 422 (a,b), 459 (d), 676 (g). Reproduced from The Huntington Library, San Marino, California; STC (2nd ed.) / 19189.
A key consideration when removing the bullet was to also remove any fragments of clothing that were carried in when the bullet struck. As a musket ball was spherical, a small circle of cloth from the soldier’s clothing would potentially enter the wound. As Wiseman described, these fragments (from typically quite dirty clothing) could lead to serious consequences, including what we would now refer to as sepsis, or blood poisoning: ‘for the Bullet pierceth not any Part without carrying Rags along with it, which corrupt in the Wound … occasioning a prolonging the Cure’.
Wiseman described two instances where contaminating rags caused problems for treatment. The first was the servant of a nobleman, shot by highwaymen, ‘yet was his Gun-shot more vexatious then all the rest, until I extracted the Bullet, and Rags carried in with it … I united and healed it in ten or twelve days, which I doubt would not have been cured in three months.’ Similarly, a wounded soldier, shot in the shoulder was treated by Wiseman: ‘After several unsuccessfull Applications, I made an Incision by the side of the Scapula into the Cavity, and pulled out the Rags that had been carried in by the Shot: and from that time all Accidents ceased, and the Wound cured soon after.’ Once the rags were removed, the wound could heal. Wiseman lamented that the lack of removal of rags from the wound would lead to poisoned wounds. He noted that ‘while any of the Rags remain in the Wound, it will never cure: but the extraneous bodies drawn out, there is little difficulty in the healing these Simple Wounds’.
Once the wound was cleared of the bullet and any rags or contaminants, the bullet hole itself needed to be closed. This could either be done by means of a suture (a stitch), a ligature (tying off a wound using a thread or bandage), or cauterisation (burning of tissue). Cauterisation was a debatable activity, with some practitioners from the sixteenth century onwards arguing that it did more harm than good. But it is clear from published surgical treatises that reference the civil-war period, that cauterisation was still common practice. The use of an ‘actual’ cautery was most common (an iron structure which was heated in a fire), although the use of hot oil was also practiced, especially in previous decades, although Ambroise Paré of France argued against this particular practice. Cauteries had a c.12 inch long metal shaft ending in a specific shape (either a sphere, olive shape, rounded bar, or a flat disk), depending on the requirements of the wound. Cauterisation helped both seal and sterilise the open wound, but the after effects of the severe burn could potentially be as dangerous as the wound itself.
Other methods for treating the wound were employed such as what is now termed ‘delayed primary closure’ (discussed in my previous blog), as well as poultices and ointments designed to encourage natural cleansing of the wound (a term referred to as ‘proper digestion’). The production of pus was seen as a good result, and indicative of wound healing. One of the most unusual of these digestives was a salve named ‘Oleum Catellorum’ (‘Oil of Puppies’). An ointment made by boiling newly-whelped puppies in lily oil, along with earthworms that had been clarified in white wine. Once boiled and strained, the liquid was mixed with terabinth (turpentine), and the resulting salve could be applied to a wound. How effective this salve was is not certain (and, ethically, is not something that we can test)! However, what is interesting is that the same recipe was reported as effective by both Ambroise Paré (who himself gained it from a colleague) in the 1500s and a century later by Richard Wiseman. These two authors regularly evidenced disdain of methodologies that they felt did not work.
Gunshots might also shatter bones if the bullet struck them. The descriptions of fractures from gunshots shows that the authors of medical treatises had experience of the splintering effects of a bullet striking a bone. The remedy for this was advised to be the removal of the shattered pieces of bone, possibly leading to a resection of the limb (joining the two regions either side of the break back together), if the damage was not too severe. How successful this was is not commonly recorded, but its presence as a suggested treatment itself is telling. Wiseman described one extreme case of a soldier on a ship who, ‘had his right Arm extremely shattered about two fingers breadth, on the outside above the Elbow’. Wiseman recalled that ‘I would have cut it off instantly with a Razour (for the Bone being shattered, there needed no Saw:) but the man would not suffer me to meddle with his Arm’. Wiseman described in detail the treatment of the wound (Wiseman, pp. 427–9), which included setting the shattered arm using wetted pasteboard as a cast, ‘as it dried, stiffened, and retained its shape, preserving the Fracture in the position I left it, and that with a very slack Bandage.’ The recovery took several months, but the soldier retained his arm.
If the limb could not be saved, then it would need to be amputated. This process is described in detail in Cooke’s Mellificium Chirurgie (1648). The flesh above the damaged region was cut using a sharp curved ‘dismembering’ knife, with the sharpened edge on the concave edge, so that the limb could be cut in a single movement. Cooke advised that this knife should be heated in a fire before-hand (which incidentally would have sterilised the blade). The flesh could then be pulled back, and the bone(s) severed using a sharp saw. Cooke advised that several saws should be kept to hand, in case of breakage, as speed was of the essence. Rather than cauterising blood vessels, Cooke advised that severed major vessels should be stoppered with small round buttons made of linen, and dipped in wine, then held in place by sutures or ligatures. The flesh of the stump could then be sewn shut, although the stress placed on the sutured region was possibly problematic. A better approach was to cut the flesh into pointed flaps which could be sewn against each other into a dome, but this was not adopted until later in the century. Amputation, usually undertaken while the patient was fully awake, was noted as being a last resort, but Cooke himself emphasised that ‘Dismembering is a dreadful Operation; yet necessary’. Survival of an amputation was likely to be proportionate to the prominence of the region amputated (records in later centuries note that survival was higher for removal of digits, hands/feet, or extremities of limbs, with lower survival for amputations of the thigh or upper arm). However, an extreme example of John Tinckler of Durham, a gunner at Hartlepool, who lost his sight and both his arms, and yet survived, as well as the prominence of severed limbs and hands or feet in the petitions from soldiers illustrates that it was possible to survive amputation.
The impact of these wounds was not only physical, and causing long-term implications for a wounded man’s ability to support himself and family, but it also impacted the soldier by means of the cost of the surgeon’s care. Although in many cases surgeons were in the pay of regiments on both sides (Pells), local civilian surgeons would charge for their services in garrison towns or once a soldier had been discharged from service.
The petition of Elizabeth Newum, Nottinghamshire (20 December 1645) described the cost of treatment of her late husband, Nathaniell, as ‘the sume of foure pounds or vpward to bee paid vnto the surgion and Pothecarie whom dayly come upon mee’. Elizabeth was being hounded for payment for her husband’s care, and reported being ‘forct to sell vp all that I have and soe I and my poore infant shall bee forced to beg’ in order to cover the cost of the treatment. Some treatments could last for many days, weeks, even months, and thus would incur considerable costs. Christopher Ellin of Black Notley, Essex, had reported in his petition to the Essex county sessions (1652) that he was shot with a musket ball during the Battle of Worcester (3 September 1651), which struck him: ‘…in one of his Armes of which wound he hath lyen almost ever since under the Chirurgeons hands in the Savoy Hospitall at London.’ Another example, Tobye Ganbran’s petition to the City and County of Gloucester (17 November 1643) records that he was ‘sorely hurte and wounded with a mvskett shott, and thereby constrainde to lye vnder the Surgeons hands to be cured (this sixe weekes) and is not it perfectlie cured, w[i]th the Charge thereof hath cost him a greate deale of money, as vnto the Surgeon xx s., besides attendance, diett, and other necessaries.’. Similarly, the petition of Peter Green (27 August 1646) to the Nottinghamshire county committee noted that ‘y[ou]r poor petic[i]oner was lately wounded in the belly by a shot from the Enemye whereof hee lay many weekes under the Chryrugeons hand to his great paine & charges’. The petition records that ‘(notwithstanding the Chyrugeon is yet unsatisfied for his great Care & wonderfull Curre)’. It is noteworthy that these petitions, each of which were proximal to the date of the wound, refer not so much to the disabling impact of the injury, but rather to the financial charge incurred from several weeks of treatment, which the soldier was expected to pay.

The Savoy Hospital (image copyright Eric Gruber von Arni).
Wounds from firearms required particular treatments, and these treatments appear to have been reasonably effective. Unfortunately, it is not possible to clearly gauge the ratio of how many soldiers died outright compared to those who died from their wounds, or as a result of treatment, versus those who survived. But there were clearly effective methods for dealing with some quite extreme injuries. The existence of petitions from maimed victims of gunshots many decades after the wound was inflicted, shows that seventeenth-century soldiers could both survive, and live with, significant injuries from firearms.
Primary Sources
G. Ballingall, Outlines of Military Surgery (Edinburgh: A&C Black, 1844).
W. Clowes, A Prooued Practise for all Young Chirurgians, concerning burnings with Gunpowder, and woundes made with Gunshot, Sword, Halbard, Pyke, Launce, or such other (Thomas Orwyn, 1588).
J. Cooke, Mellificium Chirurgie, or, The Marrow of many Good Authours (London, 1655).
J. Cooke, Supplementum Chirurgiae, or the supplement to the Marrow of Chyrurgerie (London, 1655).
J. Cooke, Mellificium Chirurgiae, or the Marrow of Chirurgery much enlarged (London, 1676).
T. Gale, Certain Works of Chirurgery, Newly Compiled (London, 1563).
A. Paré (T. Johnson, translation), The Workes of that Famous Chirurgion Ambrose Parey translated out of the Latine and compared with the French (London, 1634).
A. Paré (W. Hammond, translation), The Method of Curing Wounds made by Gun-shot. Also by Arrowes and Darts, with their Accidents (London, 1617).
R. Wiseman, Severall Chirurgical Treatises (London: Norton and Maycock, 1676).
J. Woodall, The path-way to the Surgions Chest (London, 1628).
J. Woodall, The Surgeons Mate or Military & Domestique Surgery (London, 1655).
Secondary Works
E. Gruber von Arni, Justice to the Maimed Soldier: Nursing, Medical Care and Welfare for Sick and Wounded Soldiers and their Families during the English Civil Wars and Interregnum, 1642-1660 (Aldershot: Ashgate, 2001).
G. Keynes (ed.) The Apologie and Treatise of Ambroise Paré, 1585 (Chicago: University of Chicago Press, 1952).
I. Pells, ‘Reassessing frontline medical practitioners of the British Civil Wars in the context of the seventeenth-century medical world’, The Historical Journal, 62:2 (2019), pp. 399–425.
S. M. Rutherford, ‘Ground-breaking pioneers or dangerous amateurs? Did early-modern surgery have any basis in medical science?’, in I. Pells (ed.), New Approaches to the Military History of the English Civil War (Stroud: Helion and Company, 2016), pp. 153–85.
S. M. Rutherford, ‘A new kind of surgery for a new kind of war: gunshot wounds and their treatment in the British Civil Wars’, in D.J. Appleby and A. Hopper (eds), Battle-Scarred: Mortality, Medical Care and Military Welfare in the British Civil Wars (Manchester: Manchester University Press, 2018), pp. 57–77.
John Balshaw's Jigge: Singing, Star-Crossed Lovers and Signing a Civil War Petition

'Meamed and Lamed': Approaching Civil War Petitions through the Lens of Disability History

‘Lost and impoverished for ever’: The effect of the Civil Wars on Local Communities as seen through Civil War Petitions

Civilian Suffering in the Civil War: the case of Tysoe in Warwickshire

'Battle-Scarred': The Civil War Petitions Summer School
The Persistent Petitioner: Mary Burden, Oliver Cromwell and the Wiltshire Justices of the Peace
‘The hungry jaws of want’ – Basing House and the Maw of War

'The endeavours of your servants': Oliver Cromwell, Military Welfare and Civil War Petitions
A Vengeful Vicar and a Martyred Mother: The Petition of James Bamlett
